[ANSWERED] Ms. Juggenmeir is a 71-year old Female who comes into your office with concerns of fatigue and dry skin. She is a retired Banker. She is AAOx4, ambulatory, and lives by herself. She does report increased
Ms. Juggenmeir is a 71-year old Female who comes into your office with concerns of fatigue and dry skin
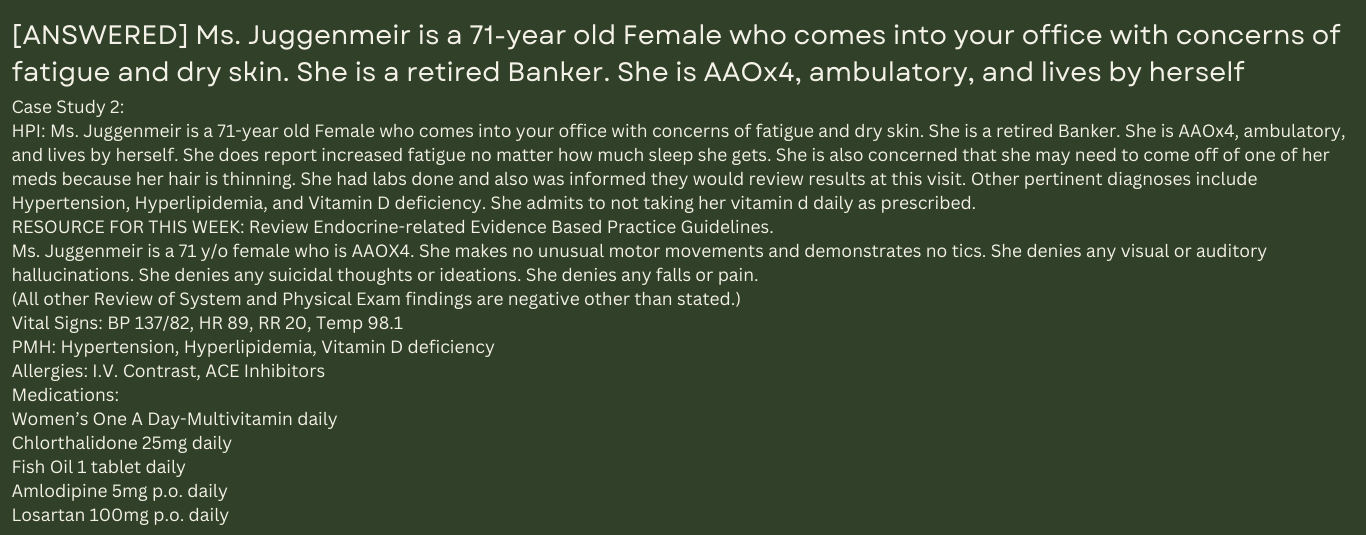
Case Study 2:
HPI: Ms. Juggenmeir is a 71–year old Female who comes into your office with concerns of fatigue and dry skin. She is a retired Banker. She is AAOx4, ambulatory, and lives by herself. She does report increased fatigue no matter how much sleep she gets. She is also concerned that she may need to come off of one of her meds because her hair is thinning. She had labs done and also was informed they would review results at this visit. Other pertinent diagnoses include Hypertension, Hyperlipidemia, and Vitamin D deficiency. She admits to not taking her vitamin d daily as prescribed.
RESOURCE FOR THIS WEEK: Review Endocrine-related Evidence Based Practice Guidelines.
Ms. Juggenmeir is a 71 y/o female who is AAOX4. She makes no unusual motor movements and demonstrates no tics. She denies any visual or auditory hallucinations. She denies any suicidal thoughts or ideations. She denies any falls or pain.
(All other Review of System and Physical Exam findings are negative other than stated.)
Vital Signs: BP 137/82, HR 89, RR 20, Temp 98.1
PMH: Hypertension, Hyperlipidemia, Vitamin D deficiency
Allergies: I.V. Contrast, ACE Inhibitors
Medications:
Women’s One A Day-Multivitamin daily
Chlorthalidone 25mg daily
Fish Oil 1 tablet daily
Amlodipine 5mg p.o. daily
Losartan 100mg p.o. daily
Atorvastatin 40mg p.o. at bedtime daily
Aspirin 81mg p.o. daily
Ergocalciferol 50,000 units PO once a month
Social History: as stated in Case Study
ROS: as stated in Case study
Diagnostics/Assessments done:
- CXR- Last cxr showed no cardiopulmonary findings. WNL
- TSH/Free T4, T3- as noted below in lab results
- Basic Metabolic Panel and CBC as shown below
- Vitamin D Level- as noted below in lab results
TEST RESULT REFERENCE RANGE
GLUCOSE 85 65-99
SODIUM 134 135-146
POTASSIUM 4.2 3.5-5.3
CHLORIDE 104 98-110
CARBON DIOXIDE 29 19-30
CALCIUM 9.0 8.6- 10.3
BUN 20 7-25
CREATININE 1.01 0.70-1.25
GLOMERULAR FILTRATION RATE (eGFR 76 >or=60 mL/min/1.73m2
TEST RESULT REFERENCE RANGE
TSH 23 0.4-4.0
FREE T4 0.05 0.9-2.4 mcg/dl
T3 3.0 2.0-4.4 ng/dl
Vitamin D 1,25 OH 14 36-144
TEST RESULT REFERENCE RANGE
WBC 7.3 3.4- 10.8
RBC 4.31 135-146
HEMOGLOBIN 14 13-17.2
HEMATOCRIT 42% 36-50
MCV 90 80-100
MCHC 34 32-36
PLATELET 272 150-400
- Subjective: What was the patient’s subjective complaint? What details did the patient provide regarding their history of present illness and personal and medical history? Include a list of prescription and over-the-counter drugs the patient is currently taking. Compare this list to the American Geriatrics Society Beers Criteria®, and consider alternative drugs if appropriate. Provide a review of systems.
- Objective: What observations did you note from the physical assessment? What were the lab, imaging, or functional assessments results?
- Assessment: Provide a minimum of three differential diagnoses. List them from top priority to least priority. Compare the diagnostic criteria for each, and explain what rules each differential in or out. Explain you critical thinking process that led you to the primary diagnosis you selected. Include pertinent positives and pertinent negatives for the specific patient case.
- Plan: Provide a detailed treatment plan for the patient that addresses each diagnosis, as applicable. Include documentation of diagnostic studies that will be obtained, referrals to other health-care providers, therapeutic interventions, education, disposition of the patient, caregiver support, and any planned follow-up visits. Provide a discussion of health promotion and disease prevention for the patient, taking into consideration patient factors, past medical history (PMH), and other risk factors. Finally, include a reflection statement on the case that describes insights or lessons learned
Expert Answer and Explanation
Diagnosis and Treatment of Hypothyroidism
Patient Information:
MJ, a 71-year-old, female, White origin
S
CC: “Fatigue and dry skin.”
HPI: MJ is a 71-year-old female of white origin who came to the office with concerns about dry skin and fatigue. She says that she has been feeling fatigued regardless of the amount of sleep she gets for the last five days. She also complains of thinning because of her meds. Associated symptoms include weight gain, constipation, increased sensitivity to cold, hoarseness, muscle weakness, muscle and joint aches, and a puffy face. She has not taken any medication to relieve the symptoms. She denies pain or falls.
Current Medications: Women’s One Day-Multivitamin daily, Fish Oil 1 tablet daily, Chlorthalidone 25mg daily, Amlodipine 5mg p.o. daily, Atorvastatin 40mg p.o. at bedtime daily, Losartan 100mg p.o. daily, Ergocalciferol 50,000 units PO once a month, and Aspirin 81mg p.o. daily
Allergies: I.V. Contrast, ACE Inhibitors
PMHx: She received the pneumonia vaccine three years ago. She does not remember information about the tetanus vaccine. Past medical illnesses include Vitamin D deficiency, Hyperlipidemia, and Hypertension.
Soc and Substance Hx: She is a retired Banker. She loves reading…
[purchase_link id=”1951″ style=”button” color=”green” text=”Access Full Answer”]
Do You Want Original Paper Written From Scratch For Similar Assignment? Click Here To Place Your Order Use Coupon Code: NEW30 to Get 30% OFF Your First Order
Use Coupon Code: NEW30 to Get 30% OFF Your First Order
Focused SOAP Note Template
Patient Information:
Initials, Age, Sex, Race
S (subjective)
CC (chief complaint): a BRIEF statement identifying why the patient is here, stated in the patient’s own words (for instance “headache,” NOT “bad headache for 3 days”).
HPI (history of present illness): This is the symptom analysis section of your note. Thorough documentation in this section is essential for patient care, coding, and billing analysis. Paint a picture of what is wrong with the patient. Use LOCATES Mnemonic to complete your HPI. You need to start EVERY HPI with age, race, and gender (e.g., 34-year-old AA male). You must include the seven attributes of each principal symptom in paragraph form not a list. If the CC was “headache”, the LOCATES for the HPI might look like the following example:
- Location: Head
- Onset: 3 days ago
- Character: Pounding, pressure around the eyes and temples
- Associated signs and symptoms: Nausea, vomiting, photophobia, phonophobia
- Timing: After being on the computer all day at work
- Exacerbating/relieving factors: Light bothers eyes; Aleve makes it tolerable but not completely better
- Severity: 7/10 pain scale
Current Medications: Include dosage, frequency, length of time used, and reason for use; also include over the counter (OTC) or homeopathic products.
Allergies: Include medication, food, and environmental allergies separately, including a description of what the allergy is (i.e., angioedema, anaphylaxis, etc.). This will help determine a true reaction versus intolerance.
PMHx: Include immunization status (note date of last tetanus for all adults), past major illnesses, and surgeries. Depending on the CC, more info is sometimes needed.
Soc and Substance Hx: Include occupation and major hobbies, family status, tobacco and alcohol use (previous and current use), and any other pertinent data. Always add some health promo question here, such as whether they use seat belts all the time or whether they have working smoke detectors in the house, living environment, text/cell phone use while driving, and support system.
Fam Hx: Illnesses with possible genetic predisposition, contagious, or chronic illnesses. Reason for death of any deceased first-degree relatives should be included. Include parents, grandparents, siblings, and children. Include grandchildren if pertinent.
Surgical Hx: Prior surgical procedures.
Mental Hx: Diagnosis and treatment. Current concerns (anxiety and/or depression). History of self-harm practices and/or suicidal or homicidal ideation.
Violence Hx: Concern or issues about safety (personal, home, community, sexual (current and historical).
Reproductive Hx: Menstrual history (date of LMP), Pregnant (yes or no), Nursing/lactating (yes or no), contraceptive use (method used), types of intercourse (oral, anal, vaginal, other, any sexual concerns).
ROS (review of symptoms): Cover all body systems that may help you include or rule out a differential diagnosis You should list each system as follows:
- General:
- Head:
- EENT (eyes, ears, nose, and throat):
- :
Note: You should list these in bullet format, and document the systems in order from head to toe.
Example of Complete ROS:
GENERAL: No weight loss, fever, chills, weakness, or fatigue.
HEENT:
- Eyes: No visual loss, blurred vision, double vision or yellow sclerae.
- Ears, Nose, Throat: No hearing loss, sneezing, congestion, runny nose, or sore throat.
SKIN: No rash or itching.
CARDIOVASCULAR: No chest pain, chest pressure or chest discomfort. No palpitations or edema.
RESPIRATORY: No shortness of breath, cough or sputum.
GASTROINTESTINAL: No anorexia, nausea, vomiting or diarrhea. No abdominal pain or blood.
GENITOURINARY: Burning on urination. Last menstrual period (LMP), MM/DD/YYYY.
NEUROLOGICAL: No headache, dizziness, syncope, paralysis, ataxia, numbness or tingling in the extremities. No change in bowel or bladder control.
MUSCULOSKELETAL: No muscle, back pain, joint pain or stiffness.
HEMATOLOGIC: No anemia, bleeding or bruising.
LYMPHATICS: No enlarged nodes. No history of splenectomy.
PSYCHIATRIC: No history of depression or anxiety.
ENDOCRINOLOGIC: No reports of sweating, cold or heat intolerance. No polyuria or polydipsia.
REPRODUCTIVE: Not pregnant and no recent pregnancy. No reports of vaginal or penile discharge. Not sexually active.
ALLERGIES: No history of asthma, hives, eczema or rhinitis.
O (objective)
Physical exam: From head-to-toe, include what you see, hear, and feel when doing your physical exam. You only need to examine the systems that are pertinent to the CC, HPI, and History. Do not use “WNL” or “normal.” You must describe what you see. Always document in head to toe format (i.e., General: Head: EENT: etc.).
Diagnostic results: Include any labs, x-rays, or other diagnostics that are needed to develop the differential diagnoses (support with evidenced and guidelines).
A (assessment)
Differential diagnoses: List a minimum of three differential diagnoses. Your primary or presumptive diagnosis should be at the top of the list. For each diagnosis, provide supportive documentation with evidence-based guidelines.
P (plan)
Includes documentation of diagnostic studies that will be obtained, referrals to other health-care providers, therapeutic interventions, education, disposition of the patient, and any planned follow up visits. Each diagnosis or condition documented in the assessment should be addressed in the plan. The details of the plan should follow an orderly manner.
Also included in this section is the reflection. Reflect on this case, and discuss what you learned, including any “aha” moments or connections you made.
Also include in your reflection, a discussion related to health promotion and disease prevention taking into consideration patient factors (such as, age, ethnic group, etc.), PMH, and other risk factors (e.g., socio-economic, cultural background, etc.).
References
You are required to include at least three evidence-based peer-reviewed journal articles or evidenced-based guidelines, which relate to this case to support your diagnostics and differentials diagnoses. Be sure to use correct APA 7th edition formatting.

Dan Palmer is a dedicated academic writing specialist with extensive experience supporting nursing students throughout their educational journey. Understanding the unique challenges faced by nursing students who balance demanding clinical rotations, family responsibilities, and rigorous coursework, Dan provides professional assignment assistance that helps students maintain academic excellence without compromising their other commitments.
With a comprehensive understanding of nursing curriculum requirements and academic standards, Dan delivers high-quality, thoroughly researched assignments that serve as valuable learning resources. His expertise spans various nursing disciplines, including clinical practice, healthcare ethics, patient care management, and evidence-based research.
Dan’s approach combines meticulous attention to detail with a commitment to timely delivery, ensuring that busy nursing students receive the support they need when they need it most. His professional assistance has helped countless nursing students successfully navigate their academic programs while maintaining their professional and personal responsibilities.
Committed to academic integrity and excellence, Dan Palmer continues to be a trusted resource for nursing students seeking reliable, professional assignment support.